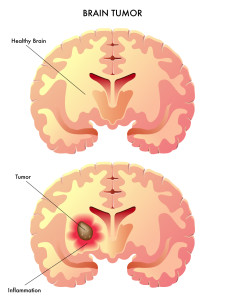
Glioblastoma, just the sound of the word can send a chill down a person’s spine and brings up the question of what exactly is it. Glioblastoma is a fast growing tumor made up of abnormal looking cells in the brain and spinal column. It usually occurs in adults and more often is located in the brain versus the spinal column. The tumor looks very different from normal healthy cells. It also overpowers healthy cells by dividing very rapidly or aggressively, taking up the space normally held by healthy cells and it takes up the blood supply and nutrients intended for the healthy cells. Glioblastoma is also known as GlioblastomaMultiforme (GBM) and Grade IV Astrocytoma. It is the most common and aggressive form of a primary brain tumor.
Glioblastoma can develop in any area of the brain and can cause a variety of symptoms including:
- Seizures
- Nausea and vomiting
- Headache
- Weakness on one side of the body only. This is called hemiparesis.
- Trouble remembering or issues with memory.
- Unexplained changes in personality
People often go to their doctors with some or all of the above symptoms and they get referred to a neurologist who can best determine what is causing the problem. The neurologist will review the patients medical history, especially the history of the symptoms, and will do a thorough physical examination. They will pay close attention to an eye examination, hearing examination and observe the patients ability to balance. In addition, coordination and reflexes will be tested to see if there are issues there as well. Patients will then be scheduled for an MRI of the brain and spinal column as well as a CT PET Scan to look for a tumor and its location. These tests can also help how much of the brains activity has been changed and look at the flow of blood going to the brain.
Once a tumor has been identified, a treatment plan will be developed and typically includes surgery to remove as much of the tumor as possible without causing significant brain damage. Patients then get a course of radiation therapy to kill any remaining cancer cells, but unfortunately radiation therapy also damages healthy tissues. Patients will also get a course of chemotherapy while they are getting the radiation. The current chemotherapy drug used for glioblastoma is Temozolomide also known as Temdar. This drug works to slow down the growth of or actually kill the cancer cells. It is a capsule usually taken once a day in the evening or at bedtime. Typically patients take the medications for 42 to 49 days and then take a break before resuming the medication once again. The oncologist will monitor how the medication is taken and give specific instructions in when to stop and when to resume the dose. The medication and radiation can cause many side effects and does not cure the Glioblastoma, it simply slows down the worsening of the disease.
Research into new, more effective treatments have been going on for years in the hopes of prolonging patients’ lives and giving them a better quality of life than the current standard therapy. There are some promising signs with ongoing studies into Nanotherapy, an Anti-Cancer Hat, a personal vaccine and gene therapy. We will take a look at each one separately.
NANOTHERAPY
Nanotherapy is a form of intra-tumoral (inside the tumor) thermotherapy (uses heat to change the temperature of core soft cell tissues). It puts a water based solution of Iron Oxide magnetic nanoparticles directly into a tumor and then heats them in an alternating flow magnetic field. The magnetic field changes directions at approximately 100,000 times per second and heats the nanoparticles up to about 176 degrees. The amount of heat generated will either damage the cancer cells so they can’t repair themselves or they will make the cancer cells more receptive and responsive to chemotherapy and radiation. In other words it fights the tumor from within the tumor itself and spares the healthy surrounding tissues. The nanoparticles are coated so they can remain in the tumor and used for repeated treatments.
Treatments are performed in a magnetic field applicator known as a Nanoactivator. The activator uses 100 Kilohertz of oscillating cool current that produces a magnetic field that rapidly moves the magnetic iron oxide particles in the field. The iron oxide is mixed in water and able to be introduced to the tumor in a syringe with simple injections and heated in the magnetic field.
This therapy is involved in a clinical trial with preliminary results available. A total of 66 patients were enrolled in the study. 59 of the patients had a recurrent glioblastoma, recurrent meaning it came back after initial treatment and stabilization. The remaining had initial diagnosis of glioblastoma. The average overall survival rate from diagnosis of tumor recurrence in 59 patients was 13.4 months. The average overall survival rate from the initial primary site diagnosis was 23.2 months. This indicates that Nanotherapy lead to longer survival times than patients on standard radiation and chemotherapy alone. There were no serious complications or side effects reported.
EF14 NOVO TTF-100A
The EF 14 Novo TTF-100A is known as the anti-cancer hat. It has been in development for over 20 years to be used as a new standard of care for glioblastoma. The phase 3 clinical trial being used to evaluate the safety and effectiveness was ended early by the Food and Drug Administration to allow more patients to receive the treatments. The initial data on this study is promising. The study followed 315 patients, 50% of the target study population. Patients were either treated with the TTF-100A and Temozolomide or just Temozolomide. The patients treated with the TTF-100A and Temozolomide had a major increase in progression free survival, compared to Temozolomide treatment alone.
- The average progression free survival for TTF-100A is 7.1 months compared to 4.0 months with Temozolomide treatment alone.
- Patients taking TTF-100A have an average overall survival rate of 19.6 months compared to 16.6 months for patients treated with Temozolomide alone.
- 43% of the patients using the TTF-100A were still alive at 2 years as opposed to 29% of the patients on temozolomide alone.
What exactly is the TTF-100A and how does it work on glioblastoma tumors? It is a low intensity, intermediate frequency alternating electrical field that sends electrical pulses into the brain through ceramic transducers located inside a white skull cap that is worn on the head for 18 hours a day. The pulsating electrical field interferes with the proteins that are involved in the cancer cell division and prevents the faster than healthy cell reproduction of cancer cells. It also causes cell death prior to division.
The TTF-100A is non-invasive and uses insulated transducer arrays placed directly on the skin that surrounds the tumor. It does not give any electric current to the healthy tissue, nor does it stimulate or heat the nerves muscles or tissues. These transducers create an electric field within the tumor that alternates between attracting and repelling the charged components of cells as the cells prepare to divide. The treatment is very portable for patients, as it is worn for a continuous period of time. They can take the equipment with them, all it requires is a portable electric field generator, the transducer arrays and rechargeable batteries. While wearing the skull cap, 4 transducer arrays target the tumor. An MRI is used to determine the correct array placement to have the best effect on the tumor.
The treatment is intended for patients over the age of 22 and is intended to be used when standard medical therapy, surgery and radiation have been exhausted. It cannot be used in the following situations:
- Active medical devices implanted
- Missing bones in the skull
- Presence of bullet fragments
- Deep brain stimulators or spinal cord stimulators
- Pacemakers, defibrillators or programmable shunts.
A benefit of this treatment is the patient can be independent and carry out a fairly normal life. There are very few side effects or risks from the treatment. The most common side effects include, skin irritation under the arrays, headaches, a feeling of weakness, falls, fatigue and muscle twitching.
DCVAX :A PERSONALIZED VACCINE
Northwest Biotherapeutics in Bethesda Maryland has been researching the effectiveness of a cancer treatment by using the patients own immune system, white blood cells, to attack the glioblastoma. In other words, the DCVax restarts an immune system weakened by cancer. Bone marrow cells that have not yet formed into immune cells are taken from the patient’s blood and grown into the dendritic, or starter white blood cells. Once the dendritic white blood cells are ready, they are introduced to the tumors biomarkers so they can seek out and destroy the specific cancer cells. Once the dendritic cells have been activated and educated in the specific tumor to attack the patient receives an injection to begin their treatment.
The DCVax has already participated in Phase 1 and 2 clinical trials with good results noted. 39 patients were enrolled in this study. 20 patients had a new or initial tumor occurrence and 19 patients had a recurrent glioblastoma tumor. The 20 newly diagnosed patients who had the DCVax had no evidence of tumor recurrence for an average of 2 years. They also had an average survival of 3 years, 2.5 times longer than the average survival for patients who had the current standard treatment alone. Results presented in July of 2011 showed 33% of the patients reached or exceeded 4 years of survival and 27% had reached or exceeded 6 years. In 2014 it was reported that 2 patients had exceeded 10 years survival.
These results have led to a large scale Phase 3 clinical trial that will look at the DCVax versus a placebo and will evaluate the safety and effectiveness. 348 patients will be enrolled in the study. There are 51 sites participating in the United States and 30 sites in the United Kingdom. To participate in the study, the patients must be greater than 22 years of age and have all screening completed before they have surgery to remove the tumor. The patients will still receive standard treatment of surgery, radiation and chemotherapy with Temozolomide. 2 out of 3 patients will receive the DCVax and 1 out of 3 patients will receive autologous PBMC, the placebo medication. Patients will receive 2 intradermal (under the skin) injections on day 0, 10, 20 and at weeks 8, 16,32,48, 72, 96 and 120. They will be checked on an ongoing basis for any signs of progression of the disease or tumor recurrence and any safety issues.
VB-111 GENE THERAPY
VBL Therapeutics has been working on a gene therapy treatment to target the cancer cells blood supply and starve them of the food they need to grow and divide. When cancer cells grow, they send out special chemical messengers that start new blood vessels to grow and feed the cancer cells the oxygen and nutrients they need. The cells that line the newly formed blood vessels have unique genetic markers that can be maneuvered and changed to decrease the blood flow to the cancer cell.
VB-111 is actually a genetically created harmless adenovirus that is capable of attacking and infecting the cells in the blood vessels feeding the tumor. A gene infection inserts itself into the blood vessel cell walls causing them to self – destruct and cut off the blood, nutrient and oxygen flow to the tumor. This prevents the cancer cell from dividing and starts a death process in the cancer cells. One advantage of this type of treatment is it preserves the healthy non-cancerous tissue and does not affect the healthy blood vessels. Other than flu-like symptoms there are few side effects.
The first trial showed good results. 46 patients, for whom other treatments had failed , were enrolled and given repeated intravenous infusions of the virus particles along with the standard therapy for a total of 18 months. There was a significant improvement in the length of survival, 3 months longer than standard therapy.
There is now a Phase 1 clinical trial underway in the United States that is looking at how the infusion works and how safe it is. 56 patients with advanced cancer are enrolled in this study and will be receiving multiple therapeutic doses and watched very carefully for a trend of improvement in the progression free survival rate and overall survival. It will be interesting to see if the results show the same trend for survival as the initial study.
All of these trials for glioblastoma show some promise for both patients newly diagnosed and patients who have a recurrence. It will be interesting to see how all four trials progress in 2015 and beyond.
Reference:
- http://www.cancer.gov/dictionary?cdrid=45698
- http://www.celldex.com/clinical-trials/brain-cancer.php
- http://www.washingtonpost.com/national/health-science/new-therapies-offer-some-hope-for-those-facing-glioblastoma-brain-tumors/2015/02/23/4f3ff3cc-981e-11e4-8005-1924ede3e54a_story.html
- http://link.springer.com/article/10.1007%2Fs11060-010-0389-0
- http://www.magforce.de/en/home.html
- http://novocure.com/~/media/Files/N/Novocure/press-release/2014/201408-EF14-Trial-Results-Press-Release.pdf
- http://novocure.com/our-therapy.aspx
- http://www.nwbio.com/dcvax-l/
- https://clinicaltrials.gov/ct2/show/NCT00045968
- http://www.vblrx.com/cancer-programs/cancer-pipline/
- http://www.vblrx.com/vbl-therapeutics-receives-fda-fast-track-designation/
- http://www.ncbi.nlm.nih.gov/pubmed/23589178
- http://globenewswire.com/news-release/2015/02/17/706910/10120403/en/VBL-Therapeutics-Announces-Removal-of-FDA-Partial-Clinical-Hold-on-VB-111.html
I needs to spend some time learning more or understanding more. Thanks for fantastic info I was looking for this information.